
Influenza, commonly known as the 'flu' , is an
infectious disease of
birds and
mammals
caused by
RNA
viruses of the family
Orthomyxoviridae, the
influenza viruses. The most common symptoms are
chills,
fever,
sore throat,
muscle
pains,
headache (often severe),
coughing,
weakness/fatigue
and
general discomfort.[1]
Although it is often confused with other
influenza-like illnesses, especially the
common cold, influenza is a more severe disease caused by a
different type of virus.[2]
Influenza may produce
nausea
and
vomiting, particularly in children,[1]
but these symptoms are more common in the unrelated
gastroenteritis, which is sometimes inaccurately referred to as
"stomach flu" or "24-hour flu".[3]
Flu can occasionally lead to
pneumonia, either direct viral pneumonia or secondary bacterial
pneumonia, even for persons who are usually very healthy.[4][5][6]
In particular it is a warning sign if a child (or presumably an adult)
seems to be getting better and then relapses with a high fever as this
relapse may be bacterial pneumonia.[7]
Another warning sign is if the person starts to have trouble breathing.[6]
Typically, influenza is
transmitted through the air by coughs or sneezes, creating
aerosols containing the virus. Influenza can also be transmitted by
direct contact with bird droppings or
nasal
secretions, or through contact with contaminated surfaces. Airborne
aerosols have been thought to cause most infections, although which
means of transmission is most important is not absolutely clear.[8]
Influenza viruses can be inactivated by
sunlight,
disinfectants and
detergents.[9][10]
As the virus can be inactivated by soap, frequent hand washing reduces
the risk of infection.[11]
Influenza spreads around the world in
seasonal epidemics, resulting in about three to five million yearly
cases of severe illness and about 250,000 to 500,000 yearly deaths,[12]
rising to millions in some
pandemic years. In the 20th century three
influenza pandemics occurred, each caused by the appearance of a new
strain of the virus in humans, and killed tens of millions of
people. Often, new influenza strains appear when an existing flu virus
spreads to humans from another animal
species,
or when an existing human strain picks up new
genes from
a virus that usually infects birds or pigs. An avian strain named
H5N1 raised the concern of a new influenza pandemic after it emerged
in Asia in the 1990s, but it has not
evolved to a form that spreads easily between people.[13]
In April 2009 a novel flu strain evolved that combined genes from human,
pig, and bird flu. Initially dubbed "swine flu" and also known as
influenza A/H1N1, it emerged in Mexico, the United States, and
several other nations. The
World Health Organization officially declared the outbreak to be a
pandemic on 11 June 2009 (see
2009 flu pandemic). The WHO's declaration of a pandemic level 6 was
an indication of spread, not severity, the strain actually having a
lower mortality rate than common flu outbreaks.[14]
Vaccinations against influenza are usually made available to people
in
developed countries.[15]
Farmed poultry is often vaccinated to avoid decimation of the flocks.[16]
The most common human vaccine is the trivalent
influenza vaccine (TIV) that contains purified and inactivated
antigens from three viral strains. Typically, this vaccine includes
material from two
influenza A virus subtypes and one
influenza B virus strain.[17]
The TIV carries no risk of transmitting the disease, and it has very low
reactivity. A vaccine formulated for one year may be ineffective in the
following year, since the influenza virus evolves rapidly, and new
strains quickly replace the older ones.
Antiviral drugs such as the
neuraminidase inhibitor
oseltamivir (Tamiflu) have been used to treat influenza;[18]
however, their effectiveness is difficult to determine due to much of
the data remaining unpublished.[19]
Signs and symptoms
Most
sensitive symptoms for diagnosing influenza[20]
| Symptom: |
sensitivity |
specificity |
| Fever |
68–86% |
25–73% |
| Cough |
84–98% |
7–29% |
| Nasal congestion |
68–91% |
19–41% |
- All three findings, especially fever, were less
sensitive in people over 60 years of age.
|

Symptoms of influenza,
[21]
with fever and cough the most common symptoms.
[20]
Approximately 33% of people with influenza are asymptomatic.[22]
Symptoms of influenza can start quite suddenly one to two days after
infection. Usually the first symptoms are chills or a chilly sensation,
but fever is also common early in the infection, with body temperatures
ranging from 38–39 °C (approximately 100–103 °F).[23]
Many people are so ill that they are confined to bed for several days,
with aches and pains throughout their bodies, which are worse in their
backs and legs.[1]
Symptoms of influenza may include:
It can be difficult to distinguish between the
common cold and influenza in the early stages of these infections,[2]
but a flu can be identified by a high fever with a sudden onset and
extreme fatigue. Diarrhea is not normally a symptom of influenza in
adults,[20]
although it has been seen in some human cases of the
H5N1 "bird flu"[28]
and can be a symptom in children.[25]
The symptoms most reliably seen in influenza are shown in the table to
the right.[20]
Since
antiviral drugs are effective in treating influenza if given early (see
treatment section, below), it can be important to identify cases
early. Of the symptoms listed above, the combinations of fever with
cough, sore throat and/or nasal congestion can improve diagnostic
accuracy.[29]
Two
decision analysis studies[30][31]
suggest that during local outbreaks of influenza, the
prevalence will be over 70%,[31]
and thus patients with any of these combinations of symptoms may be
treated with
neuraminidase inhibitors without testing. Even in the absence of a
local outbreak, treatment may be justified in the elderly during the
influenza season as long as the prevalence is over 15%.[31]
The available laboratory tests for influenza continue to improve. The
United States
Centers for Disease Control and Prevention (CDC) maintains an
up-to-date summary of available laboratory tests.[32]
According to the CDC, rapid diagnostic tests have a sensitivity of
70–75% and specificity of 90–95% when compared with
viral culture. These tests may be especially useful during the
influenza season (prevalence=25%) but in the absence of a local
outbreak, or peri-influenza season (prevalence=10%[31]).
On the more serious side, influenza can occasionally cause either
direct viral or secondary bacterial pneumonia.[5][6]
The obvious symptom is trouble breathing. In addition, if a child (or
presumably an adult) seems to be getting better and then relapses with a
high fever, that is a danger sign since this relapse can be bacterial
pneumonia.[7]
Virology
Types of virus
In
virus classification influenza viruses are
RNA viruses that make up three of the five
genera of the family
Orthomyxoviridae:[33]
These viruses are only distantly related to the
human parainfluenza viruses, which are RNA viruses belonging to the
paramyxovirus family that are a common cause of respiratory
infections in children such as
croup,[34]
but can also cause a disease similar to influenza in adults.[35]
Influenzavirus A
This genus has one species, influenza A virus. Wild aquatic birds are
the natural hosts for a large variety of influenza A. Occasionally,
viruses are transmitted to other species and may then cause devastating
outbreaks in domestic poultry or give rise to human influenza
pandemics.[36]
The type A viruses are the most virulent human pathogens among the three
influenza types and cause the most severe disease. The influenza A virus
can be subdivided into different
serotypes based on the
antibody response to these viruses.[37]
The serotypes that have been confirmed in humans, ordered by the number
of known human pandemic deaths, are:
Influenzavirus B
This genus has one species, influenza B virus. Influenza B almost
exclusively infects humans[37]
and is less common than influenza A. The only other animals known to be
susceptible to influenza B infection are the
seal[39]
and the
ferret.[40]
This type of influenza mutates at a rate 2–3 times slower than type A[41]
and consequently is less genetically diverse, with only one influenza B
serotype.[37]
As a result of this lack of
antigenic
diversity, a degree of
immunity to influenza B is usually acquired at an early age.
However, influenza B mutates enough that lasting immunity is not
possible.[42]
This reduced rate of antigenic change, combined with its limited host
range (inhibiting cross species
antigenic shift), ensures that pandemics of influenza B do not
occur.[43]
Influenzavirus C
This genus has one species, influenza C virus, which infects humans,
dogs and pigs, sometimes causing both severe illness and local
epidemics.[44][45]
However, influenza C is less common than the other types and usually
only causes mild disease in children.[46][47]
Structure, properties, and subtype nomenclature
Influenzaviruses A, B and C are very similar in overall structure.[48]
The virus particle is 80–120
nanometers in diameter and usually roughly spherical, although
filamentous forms can occur.[49][50]
These filamentous forms are more common in influenza C, which can form
cordlike structures up to 500 micrometers
long on the surfaces of infected cells.[51]
However, despite these varied shapes, the viral particles of all
influenza viruses are similar in composition.[51]
These are made of a
viral envelope containing two main types of
glycoproteins, wrapped around a central core. The central core
contains the viral
RNA
genome
and other viral proteins that package and protect this RNA. RNA tends to
be single stranded but in special cases it is double.[50]
Unusually for a virus, its genome is not a single piece of
nucleic acid; instead, it contains seven or eight pieces of
segmented
negative-sense RNA, each piece of RNA containing either one or two
genes,
which code for a gene product (protein).[51]
For example, the influenza A genome contains 11 genes on eight pieces of
RNA, encoding for 11
proteins:
hemagglutinin (HA),
neuraminidase (NA),
nucleoprotein (NP),
M1,
M2,
NS1, NS2(NEP: nuclear export protein), PA, PB1 (polymerase basic 1),
PB1-F2 and PB2.[52]
Hemagglutinin (HA) and neuraminidase (NA) are the two large
glycoproteins on the outside of the viral particles. HA is a
lectin
that mediates binding of the virus to target cells and entry of the
viral genome into the target cell, while NA is involved in the release
of progeny virus from infected cells, by cleaving sugars that bind the
mature viral particles.[53]
Thus, these proteins are targets for
antiviral drugs.[54]
Furthermore, they are
antigens
to which
antibodies can be raised. Influenza A viruses are classified into
subtypes based on antibody responses to HA and NA. These different types
of HA and NA form the basis of the H and N distinctions
in, for example, H5N1.[55]
There are 16 H and 9 N subtypes known, but only H 1, 2 and 3, and N 1
and 2 are commonly found in humans.[56]
Replication

Host cell invasion and replication by the influenza virus.
The steps in this process are discussed in the text.
Viruses can replicate only in living cells.[57]
Influenza infection and replication is a multi-step process: First, the
virus has to bind to and enter the cell, then deliver its genome to a
site where it can produce new copies of viral proteins and RNA, assemble
these components into new viral particles, and, last, exit the host
cell.[51]
Influenza viruses bind through
hemagglutinin onto
sialic acid sugars on the surfaces of
epithelial cells, typically in the nose, throat, and
lungs of
mammals, and
intestines of birds (Stage 1 in infection figure).[58]
After the hemagglutinin is
cleaved by a
protease, the cell imports the virus by
endocytosis.[59]
The intracellular details are still being elucidated. It is known
that virions converge to the
microtubule organizing center, interact with acidic endosomes and
finally enter the target endosomes for genome release.[60]
Once inside the cell, the acidic conditions in the
endosome cause two events to happen: First, part of the
hemagglutinin protein fuses the
viral envelope with the vacuole's membrane, then the M2
ion channel allows
protons
to move through the viral envelope and acidify the core of the virus,
which causes the core to dissemble and release the viral RNA and core
proteins.[51]
The viral RNA (vRNA) molecules, accessory proteins and
RNA-dependent RNA polymerase are then released into the
cytoplasm (Stage 2).[61]
The M2 ion channel is blocked by
amantadine drugs, preventing infection.[62]
These core proteins and vRNA form a complex that is transported into
the
cell nucleus, where the RNA-dependent RNA polymerase begins
transcribing complementary positive-sense vRNA (Steps 3a and b).[63]
The vRNA either is exported into the cytoplasm and translated (step 4)
or remains in the nucleus. Newly synthesized viral proteins are either
secreted through the
Golgi apparatus onto the cell surface (in the case of neuraminidase
and hemagglutinin, step 5b) or transported back into the nucleus to bind
vRNA and form new viral genome particles (step 5a). Other viral proteins
have multiple actions in the host cell, including degrading cellular
mRNA and using the released
nucleotides for vRNA synthesis and also inhibiting
translation of host-cell mRNAs.[64]
Negative-sense vRNAs that form the
genomes
of future viruses, RNA-dependent RNA polymerase, and other viral
proteins are assembled into a virion. Hemagglutinin and neuraminidase
molecules cluster into a bulge in the cell membrane. The vRNA and
viral core
proteins leave the nucleus and enter this membrane protrusion (step 6).
The mature virus buds off from the cell in a sphere of host
phospholipid membrane, acquiring hemagglutinin and neuraminidase
with this membrane coat (step 7).[65]
As before, the viruses adhere to the cell through hemagglutinin; the
mature viruses detach once their
neuraminidase has cleaved sialic acid residues from the host cell.[58]
After the release of new influenza viruses, the host cell dies.
Because of the absence of RNA
proofreading enzymes, the RNA-dependent RNA polymerase that copies
the viral genome makes an error roughly every 10 thousand nucleotides,
which is the approximate length of the influenza vRNA. Hence, the
majority of newly manufactured influenza viruses are mutants; this
causes
antigenic drift, which is a slow change in the antigens on the viral
surface over time.[66]
The separation of the genome into eight separate segments of vRNA allows
mixing or
reassortment of vRNAs if more than one type of influenza virus
infects a single cell. The resulting rapid change in viral genetics
produces
antigenic shifts, which are sudden changes from one antigen to
another. These sudden large changes allow the virus to infect new host
species and quickly overcome protective immunity.[55]
This is important in the emergence of pandemics, as discussed below in
the section on
Epidemiology.
Mechanism
Transmission
Influenza virus shedding (the time during which a person might be
infectious to another person) begins the day before symptoms appear and
virus is then released for between 5 to 7 days, although some people may
shed virus for longer periods. People who contract influenza are most
infective between the second and third days after infection.[67]
The amount of virus shed appears to correlate with fever, with higher
amounts of virus shed when temperatures are highest.[68]
Children are much more infectious than adults and shed virus from just
before they develop symptoms until two weeks after infection.[67][69]
The transmission of influenza can be
modeled mathematically, which helps predict how the virus will
spread in a population.[70]
Influenza can be spread in three main ways:[71][72]
by direct transmission (when an infected person sneezes mucus directly
into the eyes, nose or mouth of another person); the airborne route
(when someone inhales the
aerosols produced by an infected person coughing, sneezing or
spitting) and through hand-to-eye, hand-to-nose, or hand-to-mouth
transmission, either from contaminated surfaces or from direct personal
contact such as a hand-shake. The relative importance of these three
modes of transmission is unclear, and they may all contribute to the
spread of the virus.[8][73]
In the airborne route, the droplets that are small enough for people to
inhale are 0.5 to 5 µm
in diameter and inhaling just one droplet might be enough to cause an
infection.[71]
Although a single sneeze releases up to 40,000 droplets,[74]
most of these droplets are quite large and will quickly settle out of
the air.[71]
How long influenza survives in airborne droplets seems to be influenced
by the levels of
humidity and
UV radiation: with low humidity and a lack of sunlight in winter
aiding its survival.[71]
As the influenza virus can persist outside of the body, it can also
be transmitted by contaminated surfaces such as banknotes,[75]
doorknobs, light switches and other household items.[1]
The length of time the virus will persist on a surface varies, with the
virus surviving for one to two days on hard, non-porous surfaces such as
plastic or metal, for about fifteen minutes from dry paper tissues, and
only five minutes on skin.[76]
However, if the virus is present in mucus, this can protect it for
longer periods (up to 17 days on banknotes).[71][75]
Avian influenza viruses can survive indefinitely when frozen.[77]
They are inactivated by heating to 56 °C (133 °F) for a minimum of 60
minutes, as well as by acids (at pH <2).[77]
Pathophysiology

The different sites of infection (shown in red) of
seasonal H1N1 versus
avian H5N1. This influences their lethality and ability
to spread.
The mechanisms by which influenza infection causes symptoms in humans
have been studied intensively. One of the mechanisms is believed to be
the inhibition of
adrenocorticotropic hormone (ACTH) resulting in lowered
cortisol levels.[78]
Knowing which genes are carried by a particular strain can help predict
how well it will infect humans and how severe this infection will be
(that is, predict the strain's
pathophysiology).[45][79]
For instance, part of the process that allows influenza viruses to
invade cells is the
cleavage of the viral
hemagglutinin protein by any one of several human
proteases.[59]
In mild and avirulent viruses, the structure of the hemagglutinin means
that it can only be cleaved by proteases found in the throat and lungs,
so these viruses cannot infect other tissues. However, in highly
virulent strains, such as H5N1, the hemagglutinin can be cleaved by a
wide variety of proteases, allowing the virus to spread throughout the
body.[79]
The viral hemagglutinin protein is responsible for determining both
which species a strain can infect and where in the human
respiratory tract a strain of influenza will bind.[80]
Strains that are easily transmitted between people have hemagglutinin
proteins that bind to receptors in the upper part of the respiratory
tract, such as in the nose, throat and mouth. In contrast, the highly
lethal H5N1 strain binds to receptors that are mostly found deep in the
lungs.[81]
This difference in the site of infection may be part of the reason why
the H5N1 strain causes severe viral pneumonia in the lungs, but is not
easily transmitted by people coughing and sneezing.[82][83]
Common symptoms of the flu such as fever, headaches, and fatigue are
the result of the huge amounts of proinflammatory
cytokines and
chemokines (such as
interferon or
tumor necrosis factor) produced from influenza-infected cells.[2][84]
In contrast to the
rhinovirus that causes the
common cold, influenza does cause tissue damage, so symptoms are not
entirely due to the
inflammatory response.[85]
This massive immune response might produce a life-threatening
cytokine storm. This effect has been proposed to be the cause of the
unusual lethality of both the H5N1 avian influenza,[86]
and the 1918 pandemic strain.[87][88]
However, another possibility is that these large amounts of cytokines
are just a result of the massive levels of viral replication produced by
these strains, and the immune response does not itself contribute to the
disease.[89]
Prevention
Vaccination

Giving an influenza vaccination
The
influenza vaccine is recommended by the
World Health Organization and United States
Center for Disease Control and Prevention for high-risk groups, such
as children, the elderly, health care workers, and people who have
chronic illnesses such as
asthma,
diabetes,
heart disease, or are immuno-compromised among others.[90][91]
In healthy adults it is modestly effective in decreasing the amount of
influenza-like symptoms in a population.[92]
Evidence is supportive of a decreased rate of influenza in children over
the age of two.[93]
In those with
chronic obstructive pulmonary disease vaccination reduces
exacerbations,[94]
it is not clear if it reduces asthma exacerbations.[95]
There is insufficient evidence to support a change in patient outcomes
via immunizing health care workers.[96]
This includes health care workers who care for the elderly.[97]
Evidence supports a lower rate of influenza-like illness in many groups
who are immunocompromised such as those with:
HIV/AIDS,
cancer,
and post organ transplant.[98]
Due to the high
mutation rate of the virus, a particular influenza vaccine usually
confers protection for no more than a few years. Every year, the World
Health Organization predicts which strains of the virus are most likely
to be circulating in the next year (see
Historical annual reformulations of the influenza vaccine), allowing
pharmaceutical companies to develop vaccines that will provide the
best immunity against these strains.[99]
The vaccine is reformulated each season for a few specific flu strains
but dose not include all the strains active in the world during that
season. It takes about six months for the manufacturers to formulate and
produce the millions of doses required to deal with the seasonal
epidemics; occasionally, a new or overlooked strain becomes prominent
during that time.[100]
It is also possible to get infected just before vaccination and get sick
with the strain that the vaccine is supposed to prevent, as the vaccine
takes about two weeks to become effective.[101]
Vaccines can cause the
immune system to react as if the body were actually being infected,
and general infection symptoms (many cold and flu symptoms are just
general infection symptoms) can appear, though these symptoms are
usually not as severe or long-lasting as influenza. The most dangerous
adverse effect is a severe
allergic
reaction to either the virus material itself or residues from the
hen eggs used to grow the influenza; however, these reactions are
extremely rare.[102]
The cost-effectiveness of seasonal influenza vaccination has been
widely evaluated for different groups and in different settings. It has
generally been found to be a cost-effective intervention, especially in
children[103]
and the elderly,[104]
however the results of economic evaluations of influenza vaccination
have often been found to be dependent on key assumptions.[105]
Infection control
Reasonably effective ways to reduce the transmission of influenza
include good personal health and hygiene habits such as: not touching
your eyes, nose or mouth;[106]
frequent
hand washing (with soap and water, or with alcohol-based hand rubs);[107]
covering coughs and sneezes; avoiding close contact with sick people;
and staying home yourself if you are sick. Avoiding spitting is also
recommended.[108]
Although
face masks might help prevent transmission when caring for the sick,[109][110]
there is mixed evidence on beneficial effects in the community.[108][111]
Smoking raises the risk of contracting influenza, as well as producing
more severe disease symptoms.[112][113]
Since influenza spreads through both
aerosols and contact with contaminated surfaces, surface sanitizing
may help prevent some infections.[114]
Alcohol
is an effective sanitizer against influenza viruses, while
quaternary ammonium compounds can be used with alcohol so that the
sanitizing effect lasts for longer.[115]
In hospitals, quaternary ammonium compounds and
bleach
are used to sanitize rooms or equipment that have been occupied by
patients with influenza symptoms.[115]
At home, this can be done effectively with a diluted chlorine bleach.[116]
During past pandemics, closing schools, churches and theaters slowed
the spread of the virus but did not have a large effect on the overall
death rate.[117][118]
It is uncertain if reducing public gatherings, by for example closing
schools and workplaces, will reduce transmission since people with
influenza may just be moved from one area to another; such measures
would also be difficult to enforce and might be unpopular.[108]
When small numbers of people are infected, isolating the sick might
reduce the risk of transmission.[108]
Treatment
People with the flu are advised to get plenty of rest, drink plenty
of liquids, avoid using
alcohol and
tobacco and, if necessary, take medications such as acetaminophen (paracetamol)
to relieve the fever and muscle aches associated with the flu.[119]
Children and teenagers with flu symptoms (particularly fever) should
avoid taking
aspirin
during an influenza infection (especially
influenza type B), because doing so can lead to
Reye's syndrome, a rare but potentially fatal disease of the
liver.[120]
Since influenza is caused by a virus,
antibiotics have no effect on the infection; unless prescribed for
secondary infections such as
bacterial pneumonia. Antiviral medication may be effective, but some
strains of influenza can show resistance to the standard antiviral drugs
and there is concern about the quality of the research.[121]
Antivirals
The two classes of antiviral drugs used against influenza are
neuraminidase inhibitors (oseltamivir
and
zanamivir) and
M2 protein inhibitors (adamantane
derivatives). Neuraminidase inhibitors are currently preferred for flu
virus infections since they are less toxic and possibly more effective.[89]
However, their effectiveness is disputed.[19]
In 2009, the World Health Organization recommended that persons in high
risk groups, including pregnant women, children under two, and persons
with respiratory problems, begin taking antivirals as soon as they start
experiencing flu symptoms.[122][123]
Neuraminidase inhibitors
Neuraminidase inhibitors include the antiviral medications
oseltamivir (Tamiflu) and
zanamivir (Relenza). These medications may be effective against both
influenza A and B, however the confidence of the research community in
this conclusion is low as much of the trial data remains unpublished.[19][124]
Different strains of influenza viruses have differing degrees of
resistance against these antivirals, and it is impossible to predict
what degree of resistance a future pandemic strain might have.[125]
The FDA deems their effect to be modest.[19]
M2 inhibitors
The
antiviral drugs
amantadine and
rimantadine block a viral
ion channel (M2
protein) and prevent the virus from infecting cells.[62]
These drugs are sometimes effective against influenza A if given early
in the infection but are always ineffective against influenza B because
B viruses do not possess M2 molecules.[126]
Measured resistance to amantadine and rimantadine in American isolates
of
H3N2 has increased to 91% in 2005.[127]
This high level of resistance may be due to the easy availability of
amantadines as part of over-the-counter cold remedies in countries such
as China and Russia,[128]
and their use to prevent outbreaks of influenza in farmed poultry.[129][130]
The CDC recommended against using M2 inhibitors during the 2005–06
influenza season due to high levels of
drug resistance.[131]
Prognosis
Influenza's effects are much more severe and last longer than those
of the
common cold. Most people will recover completely in about one to two
weeks, but others will develop life-threatening complications (such as
pneumonia). Influenza, thus, can be deadly, especially for the weak,
young and old, or chronically ill.[55]
People with a
weak immune system, such as people with advanced
HIV infection
or transplant patients (whose immune systems are medically suppressed to
prevent transplant organ rejection), suffer from particularly severe
disease.[132]
Other high-risk groups include pregnant women and young children.[133]
The flu can worsen chronic health problems. People with emphysema,
chronic bronchitis or asthma may experience
shortness
of breath while they have the flu, and influenza may cause worsening
of
coronary heart disease or
congestive heart failure.[134]
Smoking is another
risk factor associated with more serious disease and increased
mortality from influenza.[135]
According to the World Health Organization: "Every winter, tens of
millions of people get the flu. Most are only ill and out of work for a
week, yet the elderly are at a higher risk of death from the illness. We
know the worldwide death toll exceeds a few hundred thousand people a
year, but even in developed countries the numbers are uncertain, because
medical authorities don't usually verify who actually died of influenza
and who died of a flu-like illness."[136]
Even healthy people can be affected, and serious problems from influenza
can happen at any age. People over 50 years old, very young children and
people of any age with chronic
medical conditions are more likely to get complications from
influenza, such as pneumonia,
bronchitis,
sinus, and
ear infections.[101]
In some cases, an
autoimmune response to an influenza infection may contribute to the
development of
Guillain-Barré syndrome.[137]
However, as many other infections can increase the risk of this disease,
influenza may only be an important cause during epidemics.[137][138]
This syndrome has been believed to also be a rare side effect of
influenza vaccines. One review gives an incidence of about one case per
million vaccinations.[139]
Getting infected by influenza itself increases both the risk of death
(up to 1 in 10,000) and increases the risk of developing GBS to a much
higher level than the highest level of suspected vaccine involvement
(approx. 10 times higher by recent estimates).[140][141]
Epidemiology
Seasonal
variations

Seasonal risk areas for influenza: November–April (blue),
April–November (red), and year-round (yellow).
Influenza reaches peak prevalence in winter, and because the
Northern and
Southern Hemispheres have winter at different times of the year,
there are actually two different flu seasons each year. This is why the
World Health Organization (assisted by the
National Influenza Centers) makes recommendations for two different
vaccine formulations every year; one for the Northern, and one for the
Southern Hemisphere.[99]
A long-standing puzzle has been why outbreaks of the flu occur
seasonally rather than uniformly throughout the year. Many scholars have
pondered where influenza could possibly reside during Summer in both
hemispheres. One possible explanation is that, because people are
indoors more often during the winter, they are in close contact more
often, and this promotes transmission from person to person. Increased
travel due to the Northern Hemisphere winter holiday season may also
play a role.[142]
Another factor is that cold temperatures lead to drier air, which may
dehydrate mucus, preventing the body from effectively expelling virus
particles. The virus also survives longer on surfaces at colder
temperatures and aerosol transmission of the virus is highest in cold
environments (less than 5 °C) with low relative humidity.[143]
Indeed, the lower air humidity in winter seems to be the main cause of
seasonal influenza transmission in temperate regions.[144][145]
However, seasonal changes in infection rates also occur in tropical
regions, and in some countries these peaks of infection are seen mainly
during the rainy season.[146]
Seasonal changes in contact rates from school terms, which are a major
factor in other
childhood diseases such as
measles
and
pertussis, may also play a role in the flu. A combination of these
small seasonal effects may be amplified by dynamical resonance with the
endogenous disease cycles.[147]
H5N1 exhibits seasonality in both humans and birds.[148]
An alternative hypothesis to explain seasonality in influenza
infections is an effect of
vitamin D levels on immunity to the virus.[149]
This idea was first proposed by
Robert Edgar Hope-Simpson in 1965.[150]
He proposed that the cause of influenza epidemics during winter may be
connected to seasonal fluctuations of vitamin D, which is produced in
the skin under the influence of solar (or artificial)
UV radiation. This could explain why influenza occurs mostly in
winter and during the tropical rainy season, when people stay indoors,
away from the sun, and their vitamin D levels fall.
Epidemic
and pandemic spread
As influenza is caused by a variety of species and strains of
viruses,
in any given year some strains can die out while others create
epidemics, while yet another strain can cause a
pandemic. Typically, in a year's normal two
flu
seasons (one per hemisphere), there are between three and five
million cases of severe illness and up to 500,000 deaths worldwide,
which by some definitions is a yearly influenza epidemic.[151]
Although the incidence of influenza can vary widely between years,
approximately 36,000 deaths and more than 200,000 hospitalizations are
directly associated with influenza every year in the United States.[152][153]
On average 41,400 people died each year in the United States between
1979 and 2001 from influenza.[154]
In 2010 the
Centers for Disease Control and Prevention (CDC) in the
United States changed the way it reports the 30 year estimates for
deaths. Now they are reported as a range from a low of about 3,300
deaths to a high of 49,000 per year.[155]
Roughly three times per century, a pandemic occurs, which infects a
large proportion of the world's population and can kill tens of millions
of people (see
pandemics section). One study estimated that if a strain with
similar
virulence to the
1918 influenza emerged today, it could kill between 50 and 80
million people.[156]

Antigenic shift, or reassortment, can result in novel and
highly pathogenic strains of human influenza
New influenza viruses are constantly
evolving by
mutation or by
reassortment.[37]
Mutations can cause small changes in the
hemagglutinin and
neuraminidase
antigens
on the surface of the virus. This is called
antigenic drift, which slowly creates an increasing variety of
strains until one evolves that can infect people who are immune to the
pre-existing strains. This new variant then replaces the older strains
as it rapidly sweeps through the human population, often causing an
epidemic.[157]
However, since the strains produced by drift will still be reasonably
similar to the older strains, some people will still be immune to them.
In contrast, when influenza viruses reassort, they acquire completely
new antigens—for example by reassortment between avian strains and human
strains; this is called
antigenic shift. If a human influenza virus is produced that has
entirely new antigens, everybody will be susceptible, and the novel
influenza will spread uncontrollably, causing a pandemic.[158]
In contrast to this model of pandemics based on antigenic drift and
shift, an alternative approach has been proposed where the periodic
pandemics are produced by interactions of a fixed set of viral strains
with a human population with a constantly changing set of immunities to
different viral strains.[159]

The generation time for influenza (the time from one
infection to the next) is very short (only 2 days). This
explains why influenza epidemics start and finish in a short
time scale of only a few months.
[160]
From a public health point of view, flu epidemics spread rapidly and
are very difficult to control. Most influenza virus strains are not very
infectious and each infected individual will only go on to infect one or
two other individuals (the basic reproduction number for influenza is
generally around 1.4). However, the generation time for influenza is
extremely short: the time from a person becoming infected to when he
infects the next person is only two days. The short generation time
means that influenza epidemics generally peak at around 2 months and
burn out after 3 months[clarification
needed] : the decision to intervene in an influenza
epidemic therefore has to be taken early, and the decision is therefore
often made on the back of incomplete data. Another problem is that
individuals become infectious before they become symptomatic, which
means that putting people in quarantine after they become ill is not an
effective public health intervention.[160]
For the average person, viral shedding tends to peak on day two whereas
symptoms peak on day three.[22]
History
Etymology
The word Influenza comes from the
Italian language meaning "influence" and refers to the cause of the
disease; initially, this ascribed illness to unfavorable
astrological influences.[161]
Changes in medical thought led to its modification to influenza del
freddo, meaning "influence of the cold". The word influenza
was first used in English to refer to the disease we know today in 1703
by J. Hugger of the University of Edinburgh in his thesis De Catarrho
epidemio, vel Influenza, prout in India occidentali sese ostendit.[162]
Archaic terms for influenza include epidemic catarrh, grippe
(from the French, first used by Molyneaux in 1694
[163]),
sweating sickness, and Spanish fever (particularly for the
1918 flu pandemic strain).[164]
Pandemics
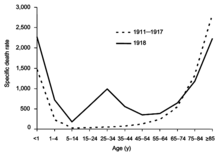
The difference between the influenza mortality age
distributions of the 1918 epidemic and normal epidemics.
Deaths per 100,000 persons in each age group, United States,
for the interpandemic years 1911–1917 (dashed line) and the
pandemic year 1918 (solid line).
[165]
The symptoms of human influenza were clearly described by
Hippocrates roughly 2,400 years ago.[166][167]
Although the virus seems to have caused epidemics throughout human
history, historical data on influenza are difficult to interpret,
because the symptoms can be similar to those of other respiratory
diseases.[168][169]
The disease may have spread from Europe to the Americas as early as the
European colonization of the Americas; since almost the entire
indigenous population of the Antilles was killed by an epidemic
resembling influenza that broke out in 1493, after the arrival of
Christopher Columbus.[170][171]
The first convincing record of an influenza pandemic was of an
outbreak in 1580, which began in Russia and spread to Europe via Africa.
In
Rome, over 8,000 people were killed, and several Spanish cities were
almost wiped out. Pandemics continued sporadically throughout the 17th
and 18th centuries, with the pandemic of 1830–1833 being particularly
widespread; it infected approximately a quarter of the people exposed.[169]
The most famous and lethal outbreak was the
1918 flu pandemic (Spanish flu pandemic) (type
A influenza,
H1N1 subtype), which lasted from 1918 to 1919. It is not known
exactly how many it killed, but estimates range from 50 to 100 million
people.[172][173][174]
This pandemic has been described as "the greatest medical holocaust in
history" and may have killed as many people as the
Black Death.[169]
This huge death toll was caused by an extremely high infection rate of
up to 50% and the extreme severity of the symptoms, suspected to be
caused by
cytokine storms.[174]
Indeed, symptoms in 1918 were so unusual that initially influenza was
misdiagnosed as dengue,
cholera,
or typhoid. One observer wrote, "One of the most striking of the
complications was hemorrhage from
mucous membranes, especially from the nose, stomach, and intestine.
Bleeding from the ears and
petechial hemorrhages in the skin also occurred."[173]
The majority of deaths were from
bacterial pneumonia, a
secondary infection caused by influenza, but the virus also killed
people directly, causing massive
hemorrhages and
edema in
the lung.[175]
The 1918 flu pandemic (Spanish flu pandemic) was truly global,
spreading even to the
Arctic
and remote
Pacific islands. The unusually severe disease killed between 2 and
20% of those infected, as opposed to the more usual flu epidemic
mortality rate of 0.1%.[165][173]
Another unusual feature of this pandemic was that it mostly killed young
adults, with 99% of pandemic influenza deaths occurring in people under
65, and more than half in young adults 20 to 40 years old.[176]
This is unusual since influenza is normally most deadly to the very
young (under age 2) and the very old (over age 70). The total mortality
of the 1918–1919 pandemic is not known, but it is estimated that 2.5% to
5% of the world's population was killed. As many as 25 million may have
been killed in the first 25 weeks; in contrast,
HIV/AIDS has killed 25 million in its first 25 years.[173]
Later flu pandemics were not so devastating. They included the 1957
Asian Flu (type A,
H2N2 strain) and the 1968
Hong Kong Flu (type A,
H3N2 strain), but even these smaller outbreaks killed millions of
people. In later pandemics
antibiotics were available to control secondary infections and this
may have helped reduce mortality compared to the Spanish Flu of 1918.[165]
The first influenza virus to be isolated was from poultry, when in
1901 the agent causing a disease called "fowl plague" was passed through
Chamberland filters, which have pores that are too small for
bacteria to pass through.[181]
The
etiological cause of influenza, the Orthomyxoviridae family of
viruses, was first discovered in
pigs by
Richard Shope in 1931.[182]
This discovery was shortly followed by the isolation of the virus from
humans by a group headed by
Patrick Laidlaw at the
Medical Research Council of
the United Kingdom in 1933.[183]
However, it was not until
Wendell Stanley first crystallized
tobacco mosaic virus in 1935 that the
non-cellular nature of viruses was appreciated.

The main types of influenza viruses in humans. Solid squares
show the appearance of a new strain, causing recurring
influenza pandemics. Broken lines indicate uncertain strain
identifications.
[184]
The first significant step towards preventing influenza was the
development in 1944 of a killed-virus vaccine for influenza by
Thomas Francis, Jr.. This built on work by Australian
Frank Macfarlane Burnet, who showed that the virus lost virulence
when it was cultured in fertilized hen's eggs.[185]
Application of this observation by Francis allowed his group of
researchers at the
University of Michigan to develop the first influenza vaccine, with
support from the
U.S. Army.[186]
The Army was deeply involved in this research due to its experience of
influenza in
World War I, when thousands of troops were killed by the virus in a
matter of months.[173]
In comparison to vaccines, the development of anti-influenza drugs has
been slower, with
amantadine being licensed in 1966 and, almost thirty years later,
the next class of drugs (the
neuraminidase inhibitors) being developed.[56]
Society and
culture
Influenza produces
direct costs due to lost
productivity and associated medical treatment, as well as
indirect costs of preventative measures. In the United States,
influenza is responsible for a total cost of over $10 billion per year,
while it has been estimated that a future pandemic could cause hundreds
of billions of dollars in direct and indirect costs.[187]
However, the economic impacts of past pandemics have not been
intensively studied, and some authors have suggested that the
Spanish influenza actually had a positive long-term effect on
per-capita income growth, despite a large reduction in the working
population and severe short-term
depressive effects.[188]
Other studies have attempted to predict the costs of a pandemic as
serious as the 1918 Spanish flu on the
U.S. economy, where 30% of all workers became ill, and 2.5% were
killed. A 30% sickness rate and a three-week length of illness would
decrease the
gross domestic product by 5%. Additional costs would come from
medical treatment of 18 million to 45 million people, and total economic
costs would be approximately $700 billion.[189]
Preventative costs are also high. Governments worldwide have spent
billions of
U.S. dollars preparing and planning for a potential H5N1 avian
influenza pandemic, with costs associated with purchasing drugs and
vaccines as well as developing
disaster drills and strategies for improved
border controls.[190]
On 1 November 2005,
United States President
George W. Bush unveiled the National Strategy to Safeguard Against
the Danger of Pandemic Influenza[191]
backed by a request to
Congress for $7.1 billion to begin implementing the plan.[192]
Internationally, on 18 January 2006, donor nations pledged US$2 billion
to combat bird flu at the two-day International Pledging Conference on
Avian and Human Influenza held in China.[193]
In an assessment of the 2009 H1N1 pandemic on selected countries in
the Southern Hemisphere, data suggest that all countries experienced
some time-limited and/or geographically isolated socio/economic effects
and a temporary decrease in tourism most likely due to fear of 2009 H1N1
disease. It is still too early to determine whether the H1N1 pandemic
has caused any long-term economic impacts.[194]
Research
Research on influenza includes studies on
molecular virology, how the virus produces disease (pathogenesis),
host
immune responses,
viral
genomics, and how the virus spreads (epidemiology).
These studies help in developing influenza countermeasures; for example,
a better understanding of the body's immune system response helps
vaccine
development, and a detailed picture of how influenza invades cells aids
the development of antiviral drugs. One important
basic
research program is the
Influenza Genome Sequencing Project, which is creating a library of
influenza sequences; this library should help clarify which factors make
one strain more lethal than another, which genes most affect
immunogenicity, and how the virus
evolves over time.[195]
Research into new vaccines is particularly important, as current
vaccines are very slow and expensive to produce and must be reformulated
every year. The sequencing of the influenza genome and
recombinant DNA technology may accelerate the generation of new
vaccine strains by allowing scientists to substitute new antigens into a
previously developed vaccine strain.[196]
New technologies are also being developed to grow viruses in
cell culture, which promises higher yields, less cost, better
quality and surge capacity.[197]
Research on a universal influenza A vaccine, targeted against the
external domain of the transmembrane viral
M2 protein (M2e), is being done at the
University of Ghent by
Walter Fiers,
Xavier Saelens and their team[198][199][200]
and has now successfully concluded Phase I clinical trials. There has
been some research success towards a "universal flu vaccine" that
produces antibodies against proteins on the viral coat which mutate less
rapidly, and thus a single shot could potentially provide longer-lasting
protection.[201][202][203]
A number of
biologics, therapeutic vaccines and immunobiologics are also being
investigated for treatment of infection caused by viruses. Therapeutic
biologics are designed to activate the immune response to virus or
antigens. Typically, biologics do not target
metabolic pathways like anti-viral drugs, but stimulate immune cells
such as
lymphocytes,
macrophages, and/or
antigen presenting cells, in an effort to drive an immune response
towards a
cytotoxic effect against the virus. Influenza models, such as murine
influenza, are convenient models to test the effects of prophylactic and
therapeutic biologics. For example,
Lymphocyte T-Cell Immune Modulator inhibits viral growth in the
murine model of influenza.[204]
In other animals
H5N1
 |
|
|
|
|
Influenza infects many animal species, and transfer of viral strains
between species can occur.
Birds are
thought to be the main
animal reservoirs of influenza viruses.[205]
Sixteen forms of
hemagglutinin and nine forms of
neuraminidase have been identified. All known subtypes (HxNy) are
found in birds, but many subtypes are endemic in humans,
dogs,
horses,
and pigs;
populations of
camels,
ferrets,
cats,
seals,
mink, and
whales
also show evidence of prior infection or exposure to influenza.[42]
Variants of flu virus are sometimes named according to the species the
strain is endemic in or adapted to. The main variants named using this
convention are:
Bird Flu,
Human
Flu,
Swine Flu,
Horse Flu and
Dog Flu. (Cat
flu generally refers to
Feline viral rhinotracheitis or
Feline calicivirus and not infection from an influenza virus.) In
pigs, horses and dogs, influenza symptoms are similar to humans, with
cough, fever and
loss of appetite.[42]
The frequency of animal diseases are not as well-studied as human
infection, but an outbreak of influenza in harbor seals caused
approximately 500 seal deaths off the
New England coast in 1979–1980.[206]
On the other hand, outbreaks in pigs are common and do not cause severe
mortality.[42]
Vaccines have also been developed to protect
poultry
from
avian influenza. These vaccines can be effective against multiple
strains and are used either as part of a preventative strategy, or
combined with
culling
in attempts to eradicate outbreaks.[207]
Bird flu
Flu symptoms in birds are variable and can be unspecific.[208]
The symptoms following infection with low-pathogenicity avian influenza
may be as mild as ruffled feathers, a small reduction in egg production,
or
weight loss combined with minor
respiratory disease.[209]
Since these mild symptoms can make diagnosis in the field difficult,
tracking the spread of
avian influenza requires laboratory testing of samples from infected
birds. Some strains such as Asian
H9N2 are highly virulent to poultry and may cause more extreme
symptoms and significant mortality.[210]
In its most highly pathogenic form, influenza in
chickens
and
turkeys produces a sudden appearance of severe symptoms and almost
100% mortality within two days.[211]
As the virus spreads rapidly in the crowded conditions seen in the
intensive farming of chickens and turkeys, these outbreaks can cause
large economic losses to poultry farmers.
An avian-adapted, highly pathogenic strain of H5N1 (called HPAI
A(H5N1), for "highly pathogenic avian influenza virus of type A of
subtype H5N1") causes
H5N1 flu, commonly known as "avian influenza" or simply "bird flu",
and is
endemic in many bird populations, especially in
Southeast Asia. This Asian lineage strain of HPAI A(H5N1) is
spreading globally. It is
epizootic (an epidemic in non-humans) and panzootic (a disease
affecting animals of many species, especially over a wide area), killing
tens of millions of birds and spurring the
culling
of hundreds of millions of other birds in an attempt to control its
spread. Most references in the media to "bird flu" and most references
to H5N1 are about this specific strain.[212][213]
At present, HPAI A(H5N1) is an avian disease, and there is no
evidence suggesting efficient human-to-human transmission of HPAI
A(H5N1). In almost all cases, those infected have had extensive physical
contact with infected birds.[214]
In the future, H5N1 may mutate or reassort into a strain capable of
efficient human-to-human transmission. The exact changes that are
required for this to happen are not well understood.[215]
However, due to the high lethality and
virulence of H5N1, its
endemic presence, and its large and increasing biological host
reservoir, the H5N1 virus was the world's pandemic threat in the 2006–07
flu season, and billions of dollars are being raised and spent
researching H5N1 and preparing for a potential influenza pandemic.[190]
Swine flu

Chinese inspectors on an airplane, checking passengers for
fevers, a common symptom of swine flu
In pigs
swine influenza produces fever, lethargy, sneezing, coughing,
difficulty breathing and decreased appetite.[216]
In some cases the infection can cause abortion. Although mortality is
usually low, the virus can produce weight loss and poor growth, causing
economic loss to farmers.[216]
Infected pigs can lose up to 12 pounds of body weight over a 3 to 4 week
period.[216]
Direct transmission of an influenza virus from pigs to humans is
occasionally possible (this is called
zoonotic swine flu). In all, 50 human cases are known to have
occurred since the virus was identified in the mid-20th century, which
have resulted in six deaths.[217]
In 2009, a swine-origin
H1N1 virus strain commonly referred to as "swine flu" caused the
2009 flu pandemic, but there is no evidence that it is endemic to
pigs (i.e. actually a swine flu) or of transmission from pigs to people,
instead the virus is spreading from person to person.[218][219]
This strain is a reassortment of several strains of H1N1 that are
usually found separately, in
humans,
birds, and pigs.[220]